.png?width=657&height=57&name=OXFORD%20LOGO%20(1).png "OXFORD LOGO (1)")

It’s been a long time since I was an English major – my working life has been focused on the world of stakeholder needs and building strategy and capability to leverage innovation, technology and science to meet those needs. So, even I was surprised when a colleague associated a quote from Hamlet as a perfect introduction to the long-running debate in healthcare today: to prevent or to treat?
Channelling Shakespeare: do we ask patients to wait and, “suffer the slings and arrows of outrageous fortune” as disease progresses, or do we proactively, “take arms against a sea of troubles and by opposing end them”, consistently monitoring patients’ well-being, and choosing to intervene early in the hope of driving healthier and longer lives?
There has been substantial discussion around this recently, particularly so in the US - the implications of the Affordable Care Act driving debate on the merits of a single payer healthcare system (and a mechanism to motivate payers to invest in true prevention – “spend now, save later”).
As we work with our healthcare clients to support the development of their brand strategies, we often find ourselves looking at ways to move stakeholders from a treatment to a prevention mindset, and it seems timely to regroup, pause for a moment, and consider the question in a little more depth.
As there are multiple ways to consider the balance between prevention and treatment – we thought we’d benefit from using the standard PESTLE to frame our thoughts.
Politics seems like a good place start
We recently worked with a client to develop a growth plan for one of their diagnostics.
The brand was already launched, with substantial uptake in some states in the US, yet minimal uptake in others.
We initially saw no obvious reason for the very stark differences in performance – an analysis of patient demographics, physician demographics, degree of need, typical attitudes towards healthcare and more didn’t provide any clues – and then we realized the map was very close to one which showed the political stance of each state.
Democratic states appeared to embrace tools to enable prevention and early detection, Republican states less so.
Never has such a stark impact of political agendas been so apparent to us, and it has, of course, significant implications for our clients’ assessment of opportunity size and field-force deployment.
Politicians are often the high-level policy makers in healthcare, and their attitudes towards prevention vs. treatment shape the policies that emerge further down the line, ultimately dictating how comprehensive an approach physicians will adopt towards implementing screening and advocating prevention.
Not surprising, patient behaviour varies widely. Many agree that undergoing testing, getting vaccinated, taking daily preventative measures, or even adapting their lifestyle are important to prevent or slow down disease.
Keeping prevention at the top of the political agenda is key to driving awareness and keeping adherence high
At the same time there are many who prefer to wait until a disease has progressed to a stage where symptoms are problematic or even to wait until the disease threatens life itself.
Today, however, we do see increasing support from the public for prevention, and greater value placed on early detection. This almost always offers an opportunity to improve outcomes.
However, when we think about interventions that are truly preventative, i.e. offered to those who are healthy, there are still many voices raising doubts around risk benefit profiles and a genuine fear of unintended long-term consequences.
We all know of the high-profile examples of policies and programs that have begun to fail, for example cervical cancer screening, or the measles, mumps and rubella vaccination program. Keeping prevention at the top of the political agenda is key to driving awareness and keeping adherence high.
Second is the economic argument
So this is one of the problems with many expensive treatments targeting later stages of disease: frankly it’s cheaper if the patient dies – especially if a costly therapy provides patients with a longer life, but not necessarily one that enables that individual to become economically productive again.
However, the economics of prevention vs. treatment are more complex. Preventing a disease from ever developing is clearly economically favorable to waiting for the disease to develop and treating it later.
But it also means there is an up-front cost now – so potentially a cash flow issue – and of course you usually must screen or treat far more individuals than would ever actually develop the disease if left alone.
Statins, for example, have been proven to decrease the risk of heart attacks and strokes significantly in both clinical trials and real-world settings across a variety of patient populations. With that reduction in risk comes an associated cost saving over the long term; one set of data measuring economic outcomes gathered by Pfizer is shown in figure 1
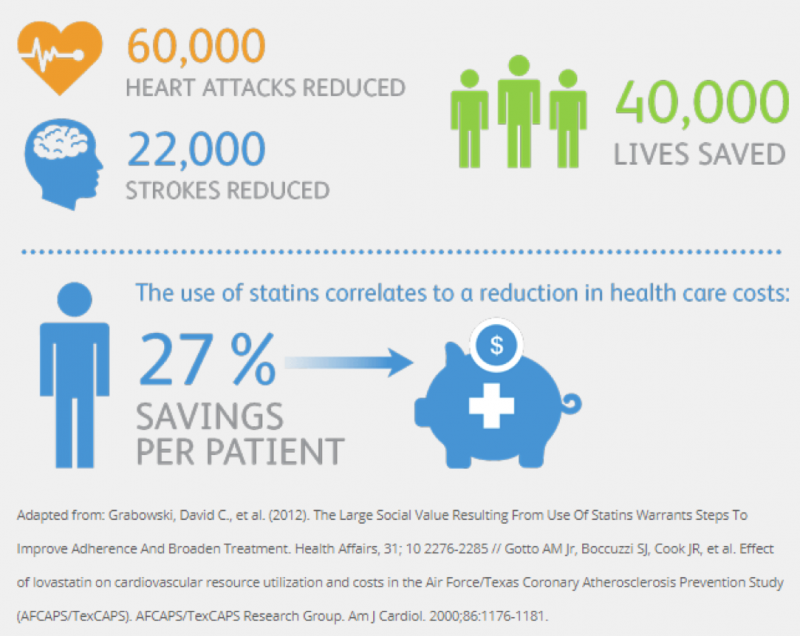
Of course, in the case of cardiovascular disease any kind of event such as a heart attack or stroke is likely to involve significant hospital costs, so it may be easy to see why the economic argument in favor of statins as a preventative treatment works.
The case for other conditions may not be so clear cut, particularly when the link between cause and effect isn’t quite so obvious. In a single payer healthcare system (e.g. NHS / UK), prevention is always expected to be economically worthwhile, assuming you can address your cash flow.
The payer invests now and makes savings later. However, when healthcare systems have multiple payers, (e.g. USA), the one investing in prevention incurs the cost, and does not necessarily reap the benefit, as data shows around half of all patients tend to switch their insurance provider around once every three years.
So, where’s the economic incentive to invest in preventative measures? Not an easy issue to solve for, and one which most likely requires health providers to rethink their business model, offering and terms
So, where’s the economic incentive to invest in preventative measures? Not an easy issue to solve for, and one which most likely requires health providers to rethink their business model, offering and terms.
What’s particularly interesting today are the novel payer models beginning to emerge for gene therapies. They are borrowing their ideas from other sectors where there’s a large up-front cost that must be managed.
For example, Novartis has introduced an annuity-based model for its SMA gene therapy, Zolgensma™. At US$2.1 million, the brand, which potentially offers a cure with a single treatment, has the distinction of being the most expensive drug ever brought to market.
Novartis worked closely with payers prior to launch to create 5 year outcomes-based agreements and novel pay-over-time options, possible as one dose of Zolgensma™ is designed to replace a lifetime of chronic therapy, to convince payers both of the intrinsic value of their approach, but also to find a way to make payments manageable.
It remains to be seen how successful uptake will be, but there is certainly a willingness from payers to consider innovative models to help ensure the economics work for prevention.
“An ounce of prevention is worth a pound of cure” - Benjamin Franklin
Third comes the myriad of social drivers
We repeatedly see market research data that tells us individuals are taking more responsibility for their own health. It’s what people genuinely want to do, and everyone agrees they should exercise more, eat healthier, and stop drinking and smoking.
Clearly, it’s not always as easy as that.
For example, only recently have we seen clinical trial data to emerge suggesting the benefits of intervening with anti-VEGF therapies before diabetic retinopathy becomes symptomatic, in a bid to prevent future vision loss – but if you’re a diabetic patient struggling to manage many different aspects of your disease, will you really prioritize a regular injection to protect eyesight that you currently have no problems with?
social change comes slowly, but steadily, and there is certainly a willingness to accept and adhere to preventative therapies in at least some disease areas today
Genuine behaviour change only comes when it is reinforced on a variety of fronts. It’s been interesting to see the attitudes towards obesity, for example, change as Novo Nordisk mounts its campaign to increase acceptance and reduce the stigma associated with diagnosis and treatment.
As well as product innovation (think liraglutide and semaglutide, as well as other compounds at earlier stages of development), Novo Nordisk is also leading the way by investing in education programs to engage physicians and improve access with sponsorship of the “Treat and Reduce Obesity Act”. It is also raising the status of obesity specialists by sponsoring academic positions and lobbying for a formal recognition of the specialty by 2020.
A more mature example is the change in social attitudes seen towards the treatment of HIV to prevent the development of AIDS. What began with campaigns in the late 1980s to raise awareness, has evolved to an expectation of disease management using antiretroviral therapy to both treat the HIV positive patient and prevent further infection. Today there is even a demand to go further to protect people without HIV but at high risk of becoming infected with the disease. Known as pre-exposure prophylaxis, drugs such as Truvada™ have been successfully launched, enabling HIV negative people to protect themselves by taking the medicine daily as well as using safer sex practices.
So social change comes slowly, but steadily, and there is certainly a willingness to accept and adhere to preventative therapies in at least some disease areas today; although key seems to be an accurate assessment of high risk, which makes an intervention truly worthwhile.
Fourth are the advances in technology
There has been an explosion in technical advances recently, with multiple biomarkers identified to help assess risk, predict, diagnose and monitor disease progression.
The availability of big data, often gathered through integrated wearables and connected mobile applications, and the development of AI powered data analysis tools, have further improved the performance of new diagnostics.
today we have the technical ability to be far more proactive in terms of screening patients or diagnosing disease at its very earliest stages
As a result, today we have the technical ability to be far more proactive in terms of screening patients or diagnosing disease at its very earliest stages.
However, these technical advances also require the means to embed new approaches into the day to day healthcare practices adopted by primary care physicians and hospitals - workflows which today often appear to have little capacity for change.
The variances in new-born screening programs around the world are easy to see.
However, uptake can be startlingly different with ease of use often the underlying reason for adopting tests which are perhaps less sensitive or less specific than others that might results in better outcomes through more targeted interventions.
There are also examples, however, of rapid uptake driven by public demand. For example, we have all seen the upsetting news headlines about deaths cause by food allergies. While tougher labelling on foods we buy from stores and restaurants is still required, technology has started to offer some help.
NIMA™ is one example of a newly developed, portable food sensor, which enables people to discern if there are peanut or gluten traces in their food in a matter of minutes via a simple test, therefore preventing a serious health event and reduce anxiety about the food they are eating.
Often these new advances in technology are embraced by pharma companies as added value solutions which can sit alongside the brand as part of the wider value proposition.
Never has the need to co-create the way these solutions are delivered with stakeholders been more important, and many companies are now employing design thinking to ensure technology is optimized and then actually used.
Imagine a future where every new medicine comes with its own test to determine patient eligibility, and this, in turn, helps to justify the costs for preventative therapies in high risk target groups.
Fifth is the legal debate; the ethics are challenging
The ethical considerations around prevention vs. treatment are always complex; if you intervene to prevent a disease, there will, of course, be some level of risk associated with that intervention, and perhaps some yet unknown long term, unintended consequences.
It is interesting to look here at the ethics driving the developing guidelines around the use of pre-implantation genetic testing. This is an extreme version of prevention – testing embryos generated from in vitro fertilisation and then selecting only those that meet your pre-specified criteria for implantation, effectively discarding those that have the potential for disease. Currently over 400 genetic conditions can be tested for in the UK, for example.
New tests are allowed if they meet the criteria set out by the Human Fertilisation and Embryology Authority based on how serious the condition is, the likelihood of it being transmitted, and an assessment of the quality of life of people currently living with the disease.
There have been many objections to the use of genetic screening, particularly from disability rights groups, as it may signal an intolerance of diversity and has the potential for abuse.
Certainly, decisions on where to draw the line are unclear, and continue to be debated, often in the courts of law. Recognizing parental rights to select a healthy embryo, as part of their duty of care to any child yet ensuring selection doesn’t violate Kant’s moral law and simply speaks to parental aims beyond prevention of disease, is clearly challenging.
Our expectation is that ethical consideration will continue to be explored on a case by case basis, driven by the risk / benefit profile of any preventative intervention. The principles developed in extreme situations, such as pre-implantation genetic testing, will undoubtedly influence the hurdles for adoption of truly preventative measures in the future.
And finally, we think about environmental concerns
Environmental concerns across all sectors, not just pharmaceuticals, society and at an individual level continue to be far reaching.
There is much being done and much more will be done: raw material and packaging reduction, improved manufacturing process to reduce waste, water usage and greenhouse gas, as well as responsible sourcing.
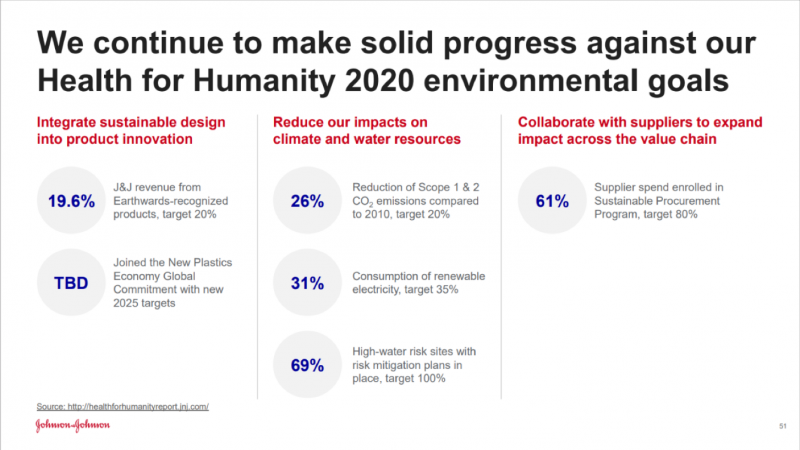
In pharmaceuticals we increasingly see examples of ‘green chemistry’, more resource-efficient and inherently safer design of molecules, materials, products, and processes which can be pursued in a wide range of contexts. Pharmaceutical companies have clear goals, which they share widely.
Figure 5 is one example we recently noticed in a J&J Investor presentation:
But how does this relate to the prevention versus treatment debate? Simply put, treatment of disease, often required for long periods of time, demands a significant volume of drugs, with their associated manufacturing and distribution needs, as well as the associated consumption of hospital resources.
So, it is easy to see that preventing disease, rather than treating disease, will always be beneficial from an environmental perspective.
So, in the end…
We all want to move to a world where preventing disease is the norm, but practically there are many, many distinctive behaviour changes required to get there. Simply said, today it’s often easier to wait and treat when necessary.
The challenges associated with each behaviour change need to be overcome on a brand by brand, issue by issue basis, and it’s a privilege to work with our clients to help to identify those challenges and develop solutions to facilitate positive behaviour change.
The message seems to be keep moving and watch this space; we think the prevention mindset will become routine in the future, as technology improves, we overcome the hurdles of implementation, prove the economics, and address the ethical concerns. Let’s do what we can to make it sooner rather than later!
If you’re considering how to move your key stakeholders from a treat to prevent mindset, or have a great case study having done so, please do get in touch.
We’d love to hear from you.
Share this

Anticipating the new drivers of behaviour in healthcare

The power of insight and partnerships in defining experiences and customer journeys

No Comments Yet
Let us know what you think